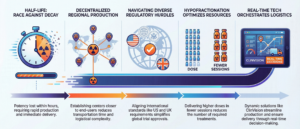
For decades, the industry has accepted a fundamental bottleneck as an inevitability: the slow, linear, and document-heavy setup of Randomization and Trial Supply Management (RTSM) systems.
The traditional RTSM deployment model is a relic of the waterfall development era – a process where technology dictates the clinical timeline rather than supporting it. However, a paradigm shift is occurring. By reversing the traditional workflow, innovative platforms are making “1-day setup” a reality, proving that the technical bottleneck is no longer a necessity, but a choice.
The "Spec-First" Bottleneck is Obsolete
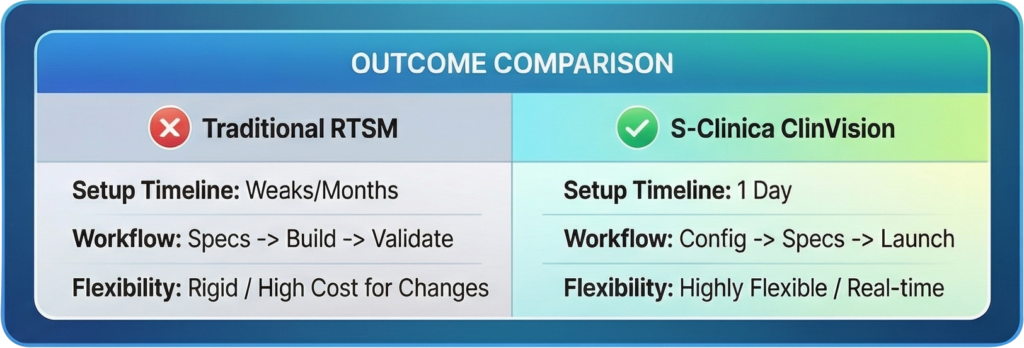
The legacy RTSM setup process follows a rigid sequence: drafting exhaustive specifications, waiting for multi-stakeholder approval, and only then beginning configuration and validation. This “spec-first” approach creates a strategic visibility black hole. Study teams are essentially flying blind, unable to see or interact with the system until the final stages of the build.
This model is inherently high-risk. When teams rely on static documents rather than functional prototypes, protocol-system misalignments often remain hidden until the User Acceptance Testing (UAT) phase. By the time these errors are discovered, the cost of correction is astronomical.
Consultant’s Reflection: The risk here isn’t just a delay; it’s a threat to trial integrity. A late-stage change during validation isn’t merely a “tweak”—it’s a massive financial hit and a strategic setback that can derail a trial’s momentum before the first patient is even randomized.
The Logic of Reversal - Configuring to Create Specs
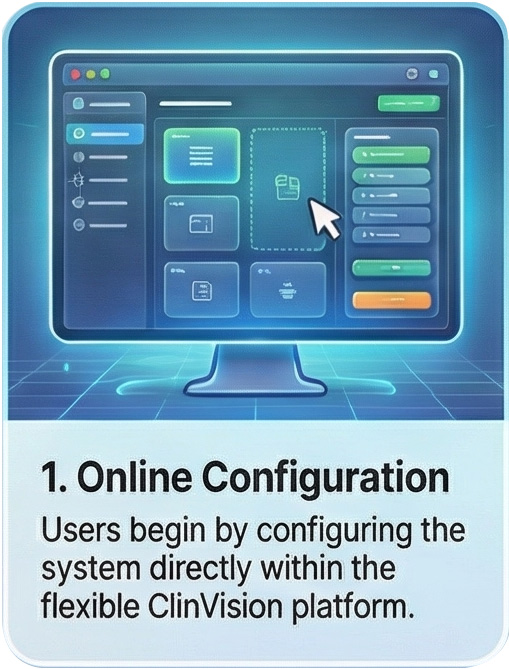
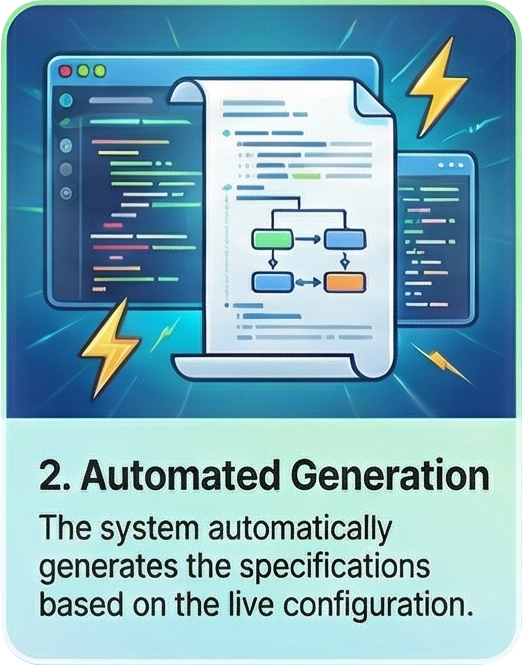
The ClinVision platform by S-Clinica disrupts this cycle by acting as a catalyst for a “reversed” workflow. Rather than waiting for written documentation to permit a build, the process begins with an immediate online configuration. In this model, the software environment is established first, allowing the system itself to generate the specifications based on the actual build.
This is the industry’s great disruptor: once those auto-generated specifications are signed, the functional RTSM is ready for deployment immediately. Crucially, this applies to studies of any complexity – shattering the myth that rapid deployment is only for simple, Phase I designs.
As soon as specifications are signed, the RTSM is generated! – study of any complexity
Consultant’s Reflection: This shift is about operational agility. By allowing configuration to drive documentation, control is handed back to the study teams. They can iterate on the trial logic in real-time, ensuring the system molds to the protocol rather than forcing the protocol to fit the software’s limitations.
RTSM Setup as a Strategic Advantage, Not a Utility
Rapid RTSM deployment has graduated from a back-office utility to a core strategic advantage. In a landscape where speed to market defines success, the ability to move from configuration to a live system in a single day creates tangible value:
- Accelerated FPI: Eliminating weeks of administrative setup translates directly into earlier patient enrollment and faster data readouts.
- Reduced Integration Friction: Flexible architectures prevent the technical “debt” and manual workarounds that plague rigid systems, ensuring higher data quality from day one.
- Operational Edge: CROs and sponsors who can deploy in 24 hours possess a level of responsiveness that traditional competitors simply cannot match.
Conclusion: The Future of Rapid Deployment
We are witnessing the end of the era where technology dictates the pace of clinical research. The shift from slow, document-heavy setups to the 1-day ClinVision model marks a turning point in clinical operations. When the “technical setup” is reduced to a single day, the primary constraint on a trial is no longer the software—it is the speed of scientific discovery itself.
As we move toward a future of increasingly complex and decentralized trials, the ability to deploy infrastructure at the speed of thought will separate the leaders from the laggards.
Closing Thought: If your RTSM setup was finished by tomorrow, how much faster could your life-saving treatment reach the patients who need it most?